Myanmar (Burma) is undergoing a complex political and economic transformation, from a long civil war and military regime to a peace process and democratisation. Since 2011, the Myanmar Ministry of Health has started to rehabilitate the fragile health system, setting the goal of achieving universal health coverage by 2030. To achieve this target, Myanmar will have to face substantial challenges; arguably one of the most important difficulties is how to allocate limited health-care resources equitably and effectively.
Objective: This study focuses on Hangzhou, a Chinese city with a population of nine million urban and rural residents, to examine the successful development and innovation experience of its primary health care service system during the new health reform in China since 2009 and then disseminate the findings through international third parties.
Methods: Measures such as data analysis, study of documents and regulations, fieldwork, and expert discussions were used to systematically investigate primary health care in Hangzhou. The findings will have a profound practical impact on the health reform for nine million rural and urban residents throughout Hangzhou’s municipal boroughs.
Results: Community health services in Hangzhou are characterized as follows: They are government led; they are guaranteed with enough financing, personnel, facilities, and regulation; supported by the unified information platform; general practitioners have been assigned the key role of health ‘gatekeepers’; they provide primary care combined with basic public health services; there are integrated urban and rural health services and insurance coverage; and there is health care‐pension‐nursing integration and general practitioner ‐ contracted ‘smart’ services. Preliminary data collection and analysis indicate that the basic health status of Hangzhou residents is superior to that of residents of China as a whole, and some health indicators in Hangzhou are comparable to those in Western developed countries.
Conclusion: It is reasonable to believe that the primary health care level in China, including Hangzhou, will be further developed and promoted with indexed performance evaluations and more effective implementation of additional measures.
Doctors, nurses and other medical staff in Myanmar are wearing black ribbons to protest the appointments of military personnel in the Ministry of Health.
“The Black Ribbon Movement Myanmar 2015,” which began on Facebook in early August, quickly amassed over 42,000 followers, and on Aug. 12, led the minister for health to drop plans to appoint military personnel to over 300 management positions within the ministry.
Writing for The Diplomat, Stanford visiting scholar Phyu Phyu Thin Zaw said the movement shows the dissatisfaction shared among her fellow doctors about the incursion of the military in the healthcare sector. She said it's also representative of greater injustices seen across Myanmar.
Four years have passed since the country transitioned from military rule toward democratization, and the Ministry of Health among other civic organizations still see the military exert influence over its operations.
Thin Zaw said she remains optimistic, though, and views the movement as a sign of the reemergence of a proactive civil society. The movement continues on this Facebook page.
The article published in TheDiplomat can be found by clicking here.
China was for hundreds of years almost entirely an agricultural society, but modern industrialization changed that dynamic, and the impact on health has been startling.
Urbanization, population aging and changes in lifestyle (from mobile to sedentary) have led a transition from an acute to chronic disease-ridden society. Now, 10 percent of China’s adult population is diabetic or pre-diabetic—holding the number one place in the world.
Feng Lin and a team of researchers want to change that reality.
Lin is part of the Corporate Affiliates Program at the Shorenstein Asia-Pacific Research Center. A visiting fellow, Lin leads a research project focused on innovations in primary health care systems in China, a topic that is also the core of his work at ACON Biotechnology. Throughout his research, Lin has worked with health policy expert Karen Eggleston.
“Thirty to forty years ago, people were talking about infectious disease,” Lin says, referring to Chinese society. “Non-communicable diseases (NCDs) like diabetes didn’t even register. They were like the black sheep in the flock.”
Now, though, Lin says that China has reached a critical stage. NCDs have a noticeable presence, and the challenge for China is to create an effective healthcare system to serve its population of 1.3 billion. Its health delivery systems are not equipped to address and prevent diseases at such a high demand.
Lin believes that improving access to care by increasing the relevance of community health care centers, improving the quality of care and integrating IT infrastructure could provide pathways forward.
In pursuit of this, he is part of the team developing an open source health index with Yaping Du, a professor at Zhejiang University, and Randall Stafford, a professor of medicine at the Stanford Prevention Research Center.
The index is one of many activities that Lin is involved with at Stanford. Forging a new type of partnership with the Asia Health Policy Program, his company sponsored a public seminar series this past year.
Determining how to restructure China’s healthcare system is a tough challenge because it’s a bureaucratic hierarchy – multiple divisions traverse each province, prefecture, township and village.
In 2009, the Chinese government laid out aggressive reforms to its healthcare policy. Lin says he believes the most essential part of that plan is the empowerment of grassroots-level community healthcare centers.
“You cannot just deal with primary level, you must look at the secondary and tertiary segments, too—a whole system approach,” he says.
Resembling a pyramid, China’s system has a finite number of top physicians who are mostly located at major hospitals. Patients who pursue services are likely to go to major hospitals in urban areas, instead of their local health community centers. About 90 percent of health care is delivered in hospitals—leading to overcrowding. Moreover, patients choose to self-treat or self-medicate which can lead to misdiagnosis.
Collecting data in Hangzhou, a coastal city just south of Shanghai (shown in map photo), Lin discovered that these trends could be explained by two reasons.
Patients have a low level of trust in community health centers, and local facilities lack capacity (e.g. having only 20 bed spaces) and expertise (e.g. employing medical personnel with sometimes outdated training). His analysis reinforced earlier outcomes found by Karen Eggleston.
Lin says the solution lies in increasing access to highly skilled physicians and organizing the system more efficiently.
Comparing China to the United States, Lin believes community healthcare centers should become main hubs for service delivery. The centers would operate as the first and last touchpoint for patient care, like “gatekeepers” in the U.S. system, administering advanced services and prevention programs like wellness education.
And while local centers are becoming more prevalent—China has more than 34,081 centers—development isn’t fast enough, not enough physicians exist, and patients aren’t actively choosing to redirect their services to community healthcare centers.
Courtesy: Feng Lin
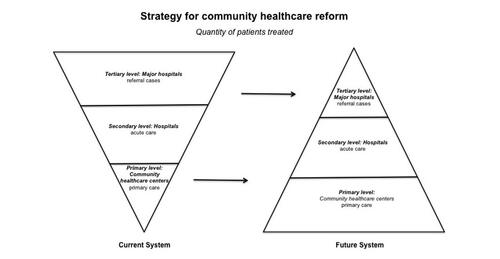
Figure 1. Strategy for community healthcare center reform advocates "strength at the grassroots." Currently patients seek care at major hospitals as their first stop, but in the future system, patients will go primarily to grassroots community healthcare centers. Courtesy: Feng Lin
Creating ease
Chinese people are typically leery of the quality of health care available at community healthcare centers, and overcoming that trust deficit won’t be an easy task. However, Lin says it’s a matter of informing citizens about local services and training more physicians to deliver quality care.
To address quality concerns, the Chinese government has set out to expand medical training programs. Enhancing the expertise of current and future physicians in rural community healthcare centers is essential, Lin says.
The health index aims to empower patients so that they can determine the best medical accommodation available, and also create a mechanism that rewards good work.
The key is to create a participatory system, one that incentivizes the patient and the physician, he says.
Hosted digitally and in the public domain, the index will list all physicians throughout Zhejiang province. Patients and healthcare professionals can login and share their experience, providing a “satisfaction rating” of hospitals and community health care centers.
Beyond external contributions, the index will support data provided by China’s national Center for Disease Control and Prevention, and local centers for disease control, to include mortality rate and cause of death and many other indicators sourced from publicly available data.
“It will build up a kind of system that people can trust – something that people can rely on,” Lin says.
Similar platforms have been implemented in advanced industrialized nations. Lin hopes that the index will offer a model that could be applied nationwide.
“It’s nearly impossible to have a single policy apply,” he says. “But, if there’s a success in one area or a few areas, the central government will pick up that approach.”
Lin expects that his team will unveil the pilot program at a conference on general practice in October 2015. The conference aims to provide practical ways to improve primary care services and the education and training of general practitioners.
Millions of women in India give birth at home, where they don’t have easy access to medical help if things go wrong. And things go wrong often. The country has one of the world’s highest rates of maternal and neonatal deaths.
To curb this problem, the government pays eligible pregnant women to deliver their babies in an accredited medical facility. With both a financial incentive and the promise of a safer childbirth, it would stand to reason that most Indian women should choose to deliver their babies in a hospital.
But that’s not the case.
Most babies are still born in homes. Early numbers from the financial incentive programs show less than half of eligible women are choosing to participate.
Stanford researchers Grant Miller and Nomita Divi think the answer to this quandary—and so many other well-intentioned policies that fall short—needs to first be considered from the perspective of patients, doctors and other health care providers. And that, they say, is a different approach than most health interventions take.
Miller and Divi are spearheading the Stanford India Health Policy Initiative, a program that seeks to rethink health interventions based on Indian health care users’ and providers’ motivations for seeking care. And to get there, the initiative’s focus comes from the people who confront these problems every day.
The program, which is connected to the International Policy Implementation Lab at Stanford’s Freeman Spogli Institute, first brings together community leaders for an in-depth discussion of where best to focus efforts. Next, teams (including students) take these recommendations and spend several months conducting fieldwork to understand health care decision-making, both from the side of patients and providers. From this foundation, the initiative produces reports detailing the behavioral motivations for why certain dimensions of health care are or are not working.
“To really understand why health policies succeed or fail, you have to see the world through the eyes of the providers and patients,” said Miller, an associate professor of medicine and a core faculty member of FSI’s Center for Health Policy and Primary Care Outcome Research. “A lot of programs are created because they seem logical from the outside. But if you don't understand a patient’s priorities or motives, your program may not work.”
Miller and Divi first applied this approach to the very issue of childbirth in India. Why weren’t more women giving birth in hospitals when there were seemingly logical reasons to do so?
Over the summer, Miller, Divi, their Indian partners, and Stanford graduate and medical students set out to answer this question. During seven weeks of field interviews and subsequent analysis, the students—with guidance from Miller and Divi —identified reasons for why Indian women weren’t accepting a stipend to have their babies in the hospital. Some of these reasons included hidden costs of delivering a baby (like the transportation cost to the hospital or unexpected medical expenses), pressure from mothers-in-law to follow tradition and deliver at home, and fear of unwanted medical procedures like Caesarean sections or sterilization.
This understanding of why patients and providers don’t always make seemingly logical health care decisions is exactly what the India Health Policy Initiative is after.
“So much academic research is driven by donors or journal articles that we read,” Miller said. “So it seemed like we were starting from the wrong place in identifying health policy challenges that we should work on.”
In January, Miller and Divi convened a group of Indian health policy leaders, health care workers, academics and entrepreneurs to understand the challenges they faced in their daily work, and what health care questions they would most like to know more about. From this two-day meeting, the group identified two focus areas for the India Health Policy Initiative over the coming year: understanding more deeply the motivations and activities of both formal and informal health care providers, and what Indians value about care from the informal sector. These informal providers are often doctors or nurses with little or no medical training that are used by many low-income Indians.
To help answer these questions and provide opportunities for students, the Stanford India Health Policy Initiative engages top students from across the university. “We want to provide our students with an experience that will hopefully shape the way they think in their future careers,” said Divi, the initiative's project manager. “And we try to achieve this by training our students to help make sense of urgent health delivery challenges, immersing them in an intensive field experience, and teaching them how to generate insights.”
To better understand providers’ motivations, as well as patients’ perspectives on both the informal and formal providers, Miller and Divi will work with this new team to carry out qualitative fieldwork this summer.
Miller explained that the approach is very anthropological.
”To be able to understand these issues, we all have to see the world through another person’s eyes, whether that be a formal or informal health provider or a patient,” he said. “This approach fundamentally relies on strong collaboration with Indian partners.”
The initiative’s teams will spend their weeks interviewing different health care providers and patients in a handful of Indian villages, taking copious notes and ultimately translating hundreds of interviews into findings.
Roshan Shankar, MS/MPP ’14, worked as part of the initiative’s team last summer, focusing on understanding pregnant women’s decisions about where to deliver their babies. After considering several summer internships with consulting firms and international organizations, Shankar declined these opportunities, instead opting to work with the Stanford India Health Policy Initiative.
Shankar is from New Delhi and has always planned to move back to his home country and work in government after school. He said the India Health Policy Initiative was a way to better understand his nation and the pressing challenges facing it.
“I’m used to sitting at a table and not venturing out,” Shankar said. “This experience showed me that things are much more different on the ground than on paper.”
After his work with the Stanford Health Policy Initiative, Shankar said he is now certain he wants to return to India and work in government.
“It was a humbling and enlightening experience. I think the way we did this entire analysis will affect the way I do any work there,” he said. “It will ensure that I do a more effective evaluation of the policies and programs that I work on, and start by going to see people who use them.”
The Stanford India Health Policy Initiative is supported by several organizations including the Center for Innovation in Global Health and the Office of International Affairs.
Abstract In 1989 more than 700 South African political prisoners went on indefinite hunger strike to protest their detention. The unprecedented scale forced the South Africian government to release hundreds of incapacitated prisoners into public hospitals and enabled the active intevention of progressive medical professionals, social workers and human rights lawyers.
The presentation explores the widespread impact of these events in galvanizing the anti-apartheid struggle, energizing international human rights organizations and propelling the new international medical protocols on the ethical care of political prisoners on hunger strike.
Nayan Shah is Professor and chair of the Department of American Studies and Ethnicity at the University of Southern california. He is the author of Contagious Divides,Epidemics and Race in San Francisco's Chinatown (Universty of California Press, 2001) and Stranger Intimacy Contesting Race Sexuality and Law in the North American West (University of California Press 2011) which was awarded the Norris and Carol Hundley Prize by the American Historical Association PAcific Branch for the most distinguished book on any historical subject. Since 2011 Shah is co-editor with Beth Freeman of GLO, The Journal of Lesbian and Gay Studies.
Co-sponsored by: American Studies, Comparative Literature. Modern Thought and Literature, History,Theater Arts and Performance Studies
Daniel and Nancy Okimoto Conference Room
Nayan Shah
Professor and Chair , Department of American Studies and Ethnicity
Speaker
University of Southern California
Patient safety is a national priority. Patient Safety Indicators (PSIs) monitor potential adverse events during hospital stays. Surgical specialty PSI benchmarks do not exist, and are needed to account for differences in the range of procedures performed, reasons for the procedure, and differences in patient characteristics. A comprehensive profile of adverse events in vascular surgery was created.
STUDY DESIGN:
The Nationwide Inpatient Sample was queried for 8 vascular procedures using ICD-9-CM codes from 2005 to 2009. Factors associated with PSI development were evaluated in univariate and multivariate analyses.
RESULTS:
A total of 1,412,703 patients underwent a vascular procedure and a PSI developed in 5.2%. PSIs were more frequent in female, nonwhite patients with public payers (p < 0.01). Patients at mid and low-volume hospitals had greater odds of developing a PSI (odds ratio [OR] = 1.17; 95% CI, 1.10-1.23 and OR = 1.69; 95% CI, 1.53-1.87). Amputations had highest PSI risk-adjusted rate and carotid endarterectomy and endovascular abdominal aortic aneurysm repair had lower risk-adjusted rate (p < 0.0001). PSI risk-adjusted rate increased linearly by severity of patient indication: claudicants (OR = 0.40; 95% CI, 0.35-0.46), rest pain patients (OR = 0.78; 95% CI, 0.69-0.90), ulcer (OR = 1.20; 95% CI, 1.07-1.34), and gangrene patients (OR = 1.85; 95% CI, 1.66-2.06).
CONCLUSIONS:
Patient safety events in vascular surgery were high and varied by procedure, with amputations and open abdominal aortic aneurysm repair having considerably more potential adverse events. PSIs were associated with black race, public payer, and procedure indication. It is important to note the overall higher rates of PSIs occurring in vascular patients and to adjust benchmarks for this surgical specialty appropriately.
BACKGROUND: Emergency department (ED) ward admissions subsequently transferred to the intensive care unit (ICU) within 24 hours have higher mortality than direct ICU admissions.
DESIGN, SETTING, PATIENTS: Describe risk factors for unplanned ICU transfer within 24 hours of ward arrival from the ED.
METHODS: Evaluation of 178,315 ED non-ICU admissions to 13 US community hospitals. We tabulated the outcome of unplanned ICU transfer by patient characteristics and hospital volume. We present factors associated with unplanned ICU transfer after adjusting for patient and hospital differences in a hierarchical logistic regression.
RESULTS: There were 4252 (2.4%) non-ICU admissions transferred to the ICU within 24 hours. Admitting diagnoses most associated with unplanned transfer, listed by descending prevalence were: pneumonia (odds ratio [OR] 1.5; 95% confidence interval [CI] 1.2–1.9), myocardial infarction (MI) (OR 1.5; 95% CI 1.2–2.0), chronic obstructive pulmonary disease (COPD) (OR 1.4; 95% CI 1.1–1.9), sepsis (OR 2.5; 95% CI 1.9–3.3), and catastrophic conditions (OR 2.3; 95% CI 1.7–3.0). Other significant predictors included: male sex, Comorbidity Points Score >145, Laboratory Acute Physiology Score
 Hangzhou, Zhejiang Province, China. Photo credit: Wikimedia Commons
Hangzhou, Zhejiang Province, China. Photo credit: Wikimedia Commons
 Courtesy: Feng Lin
Courtesy: Feng Lin